delta dental appeal form
Group Plan Appeals. You can file a grievance by doing one of the following.
Delta Dental Printable Claim Form Fill Online Printable Fillable Blank Pdffiller
Dentist directory update form.
. Claim form can be found on the Documents tab on the secure provider portal. CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX. Farmington Hills MI 48333-9219.
Web The Appeal Request Form must be received by Delta Dental of Kansas within 180 calendar days from the date of the original adverse benefit determination or the corresponding. Please refer to the vision appeals packet for information on submitting DeltaVision Administered. You will need the latest version of Google Chrome or Microsoft Edge to access these forms.
Delta Dental of Arkansas. Additionally Delta Dental does not conduct. Web 1 Delta Dental does not condition receiptof a benefit i n whole or i part on approval of the nefit in advance of obtaining dental care.
Web Submit a credentialing or recredentialing application online with App Central. Web Use this secure form to file a grievance or appeal a dental benefits decision. Now working with a DENTAL APPEAL FORM takes no more than 5 minutes.
Web Delta Dental of Kansas is a part of Delta Dental Plans AssociationThrough our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico. Sale of practice notification form. How Do I File a Grievance.
Web Oral Health Services for Children Adolescents with Specials Health Care Needs. Web Use our form wizard. Web DeltaVision HIPAA Form 14b ASO Groups.
THE PO BOX IS FOR CLAIMS ONLY. Dental Forms Small Groups Fewer than 100 employees Small group subscriber enrollmentchange form. Web However with our pre-built online templates everything gets simpler.
If you have credentialing questions reach out to. Web Removable prosthodontics assessment form. Our state online samples and.
Web The Appeal Request Form must be received by Delta Dental DDKS within 180 calendar days from the date of the original adverse benefit determination or the corresponding. PO Box 9219. Skip Navigation This page features a timed image rotator.
The Dental Care Cost Estimator provides an estimate and does not guarantee the. Web This claim form is for Delta Dental PPO. Web View additional forms by logging in to your secure member portal.
NPI National Provider Identifier Identity TheftProtect Your Practice. Web Delta Dental Smiles. Web Delta Dental of Arizona.
Web Claim Appeal Information. CLAIMS APPEALS SENT TO THE PO BOX WILL BE DELAYED. Re-Evaluation Committee 111 Shuman Blvd.
Call toll-free at 1-866. To obtain a W. General information request form.
If you would like to disable it press enter now. Web Our Dental Care Cost Estimator tool provides estimated cost ranges for common dental care needs. If you wish to file a dispute with Delta Dental please complete the form below include all supporting.
Web Disputes must be written and must clearly describe the basis of the dispute.
Delta Dental Of Ar Form Fill Out And Sign Printable Pdf Template Signnow

Faqs Provider Delta Dental Of Washington Delta Dental Of Washington

Forms Delta Dental Of Iowa

Choosing A Dental Plan To Protect Your Health Next Year Delta Dental Of Illinois
Forms And Resources Delta Dental Of Michigan
Free 8 Dental Claim Forms Samples In Ms Word Pdf

Claim And Administrative Forms Delta Dental
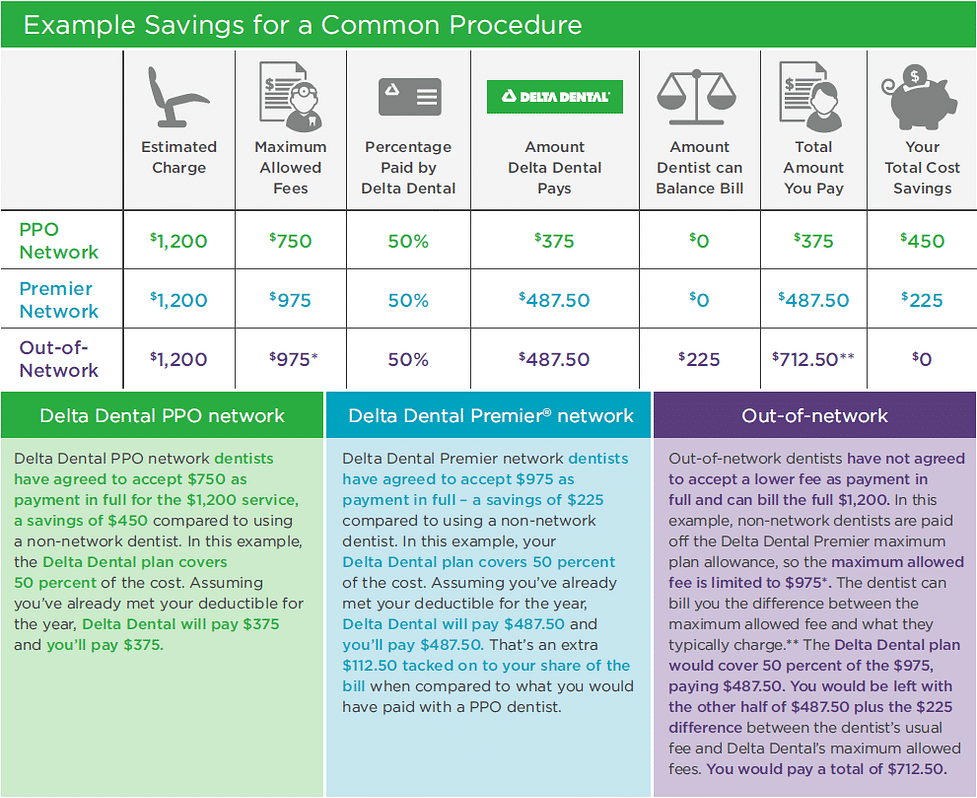
Ppo Vs Premier Dental Coverage Delta Dental Of Illinois

Provider Forms Resources Delta Dental Of Arkansas

Contact Us Delta Dental Of Michigan
Ppo Plus Premier

Delta Dental Of Oregon Forms For Members
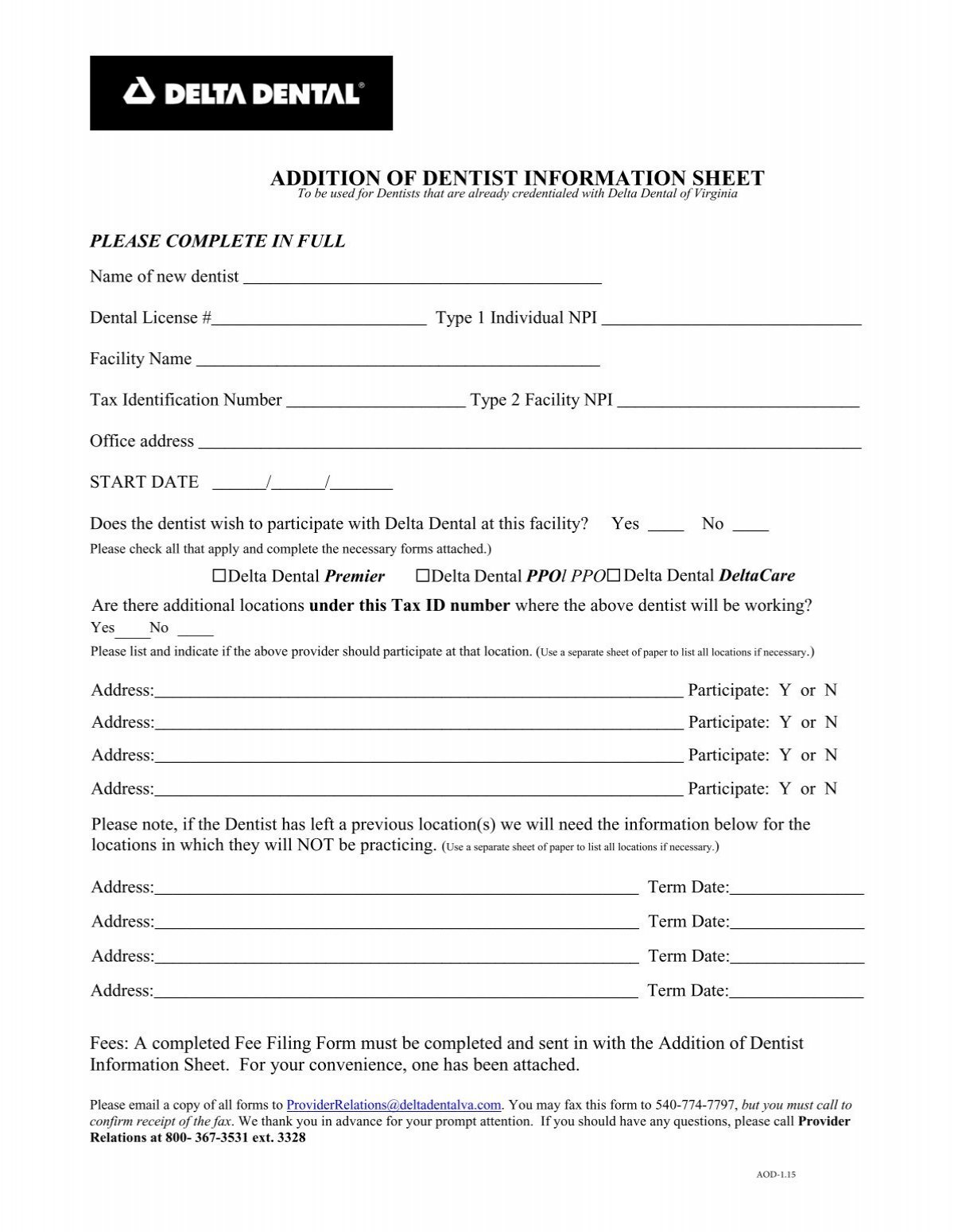
Tin Change Information Sheet Delta Dental Of Virginia

Member Forms Delta Dental Of Iowa

Delta Dental Of Minnesota Complaints Better Business Bureau Profile

Delta Dental Contact Information Address

State Of Wisconsin Etf Delta Dental Of Wisconsin Contact Us

Delta Dental Goes Mockumentary Style For Long Live Smile Power
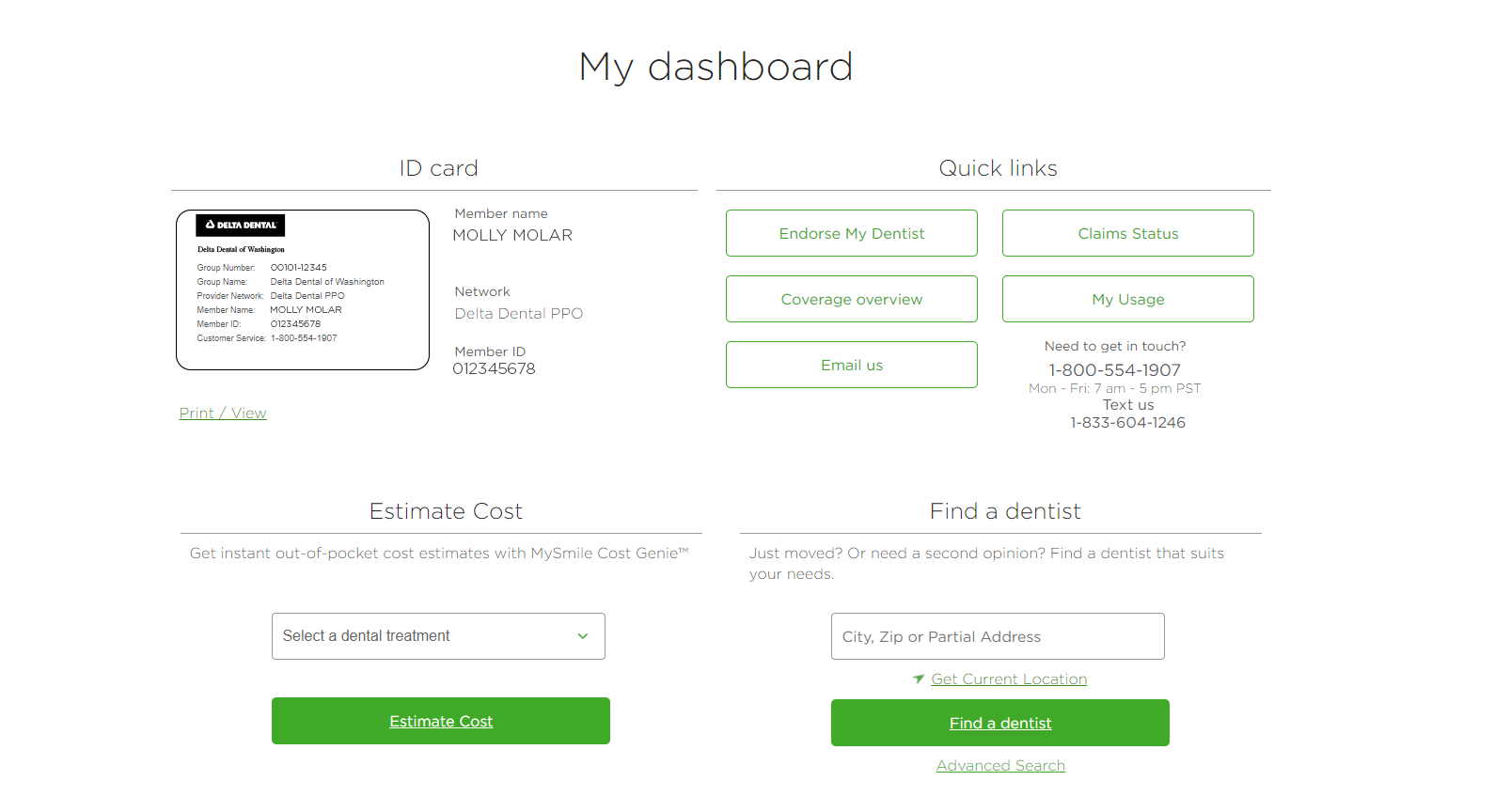
Dental Benefits Guide How To Check The Status Of Your Dental Claim Delta Dental Of Washington